What is ovulation and conception at its core, is the sequential hormonal and cellular process in which the hypothalamic-pituitary-ovarian (HPO) axis triggers a luteinizing hormone (LH) surge, causing the dominant Graafian follicle to rupture and release a mature secondary oocyte into the fallopian tube, where capacitated spermatozoa may achieve fertilization through acrosomal reaction and zona pellucida penetration, resulting in a diploid zygote. The fertilized oocyte then undergoes mitotic cleavage, progressing through morula and blastocyst stages before implanting into the decidualized endometrium approximately 6-10 days post-ovulation. For Indian women navigating this journey, understanding every phase of this process, from folliculogenesis to implantation, is the single most powerful step toward achieving a healthy pregnancy naturally.
Yet, for millions of Indian women trying to conceive, ovulation and fertilisation remain deeply mysterious. You may be tracking your cycle diligently, timing intercourse carefully, and still wondering: what is actually happening inside my body right now? This guide breaks it all down for you – step by step, in plain language, backed by science.
If you are exploring evidence-based, holistic guidance tailored specifically for women on the path to natural conception, how to conceive naturally, Gntro’s personalised preconception care platform offers clinically grounded support to help you understand and optimise your reproductive health from cycle day one.
Understanding Your Monthly Cycle: The Foundation of Fertility
Before you can understand ovulation and conception, you need to understand the menstrual cycle itself – because ovulation does not happen in isolation. It is one phase within a beautifully coordinated monthly hormonal programme.
Your menstrual cycle is governed by a dialogue between your brain and your ovaries. The hypothalamus releases gonadotropin-releasing hormone (GnRH), which signals the pituitary gland to produce two key hormones:
- Follicle-Stimulating Hormone (FSH): Stimulates the growth of ovarian follicles.
- Luteinizing Hormone (LH): Triggers the release of a mature egg.
A typical cycle lasts between 21 and 35 days, though the average is 28 days. For many Indian women, however, conditions such as polycystic ovary syndrome (PCOS), thyroid dysfunction, or nutritional deficiencies can cause irregular cycles – which directly affects ovulation timing and conception.
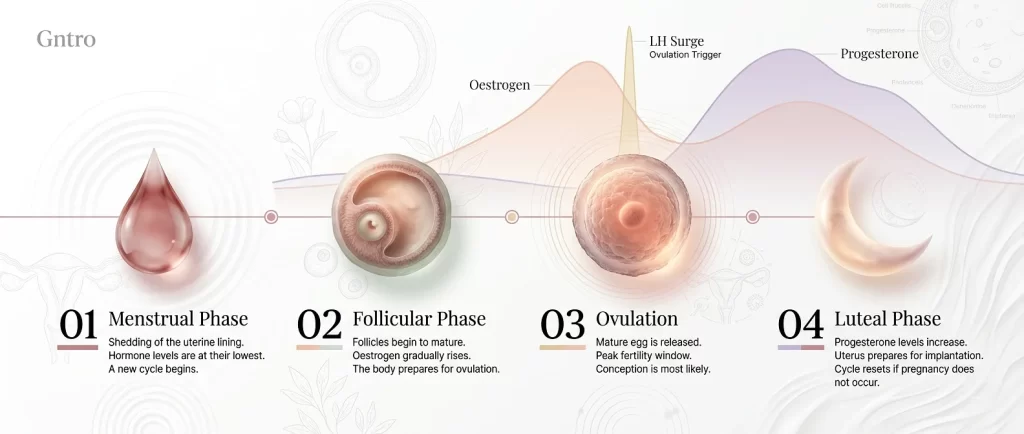
The cycle has three main phases:
| Phase | Days (28-day cycle) | Key Activity |
|---|---|---|
| Follicular Phase | Day 1-13 | Egg matures inside a follicle |
| Ovulation | Day 14 (approx.) | Egg is released |
| Luteal Phase | Day 15-28 | Uterus prepares for possible implantation |
Understanding which phase you are in at any given time is the first step toward timing conception accurately.
What is Ovulation and Conception: The Hormonal Chain Reaction
So, what is ovulation and conception in practical terms?
Ovulation is the process by which a mature egg (oocyte) is released from the ovary. This happens once per cycle – typically around day 14 of a 28-day cycle, but the exact day varies for every woman.
Conception, also called fertilisation, is the moment when a sperm cell successfully penetrates and fuses with that released egg, forming a single cell called a zygote. This zygote contains a complete set of 46 chromosomes – 23 from the egg and 23 from the sperm – and it marks the biological beginning of a new life.
The two processes are fundamentally linked. Without successful ovulation, conception is impossible. And even when ovulation occurs, conception only happens if:
- Viable sperm is present in the fallopian tube within the right time window
- The sperm successfully penetrates the egg
- The resulting embryo successfully implants in the uterine lining
According to Cleveland Clinic research on conception, in healthy couples under 35, the monthly chance of natural conception is approximately 20-25% – which is why understanding your cycle is so important.
Phase 1: Follicular Phase – How Your Eggs Mature
The journey toward ovulation begins on Day 1 of your cycle – the first day of your period.
During the follicular phase, rising FSH levels stimulate between 5 and 20 small fluid-filled sacs in your ovaries, called antral follicles, to begin developing. Each follicle contains one immature egg.
Here is what happens step by step during folliculogenesis:
- Days 1-5: Multiple follicles begin growing in response to FSH stimulation.
- Days 6-9: One follicle becomes dominant – this is called the Graafian follicle. The others stop developing and are reabsorbed.
- Days 10-13: The dominant follicle continues growing (reaching 18-24mm) and produces increasing amounts of oestradiol (estrogen).
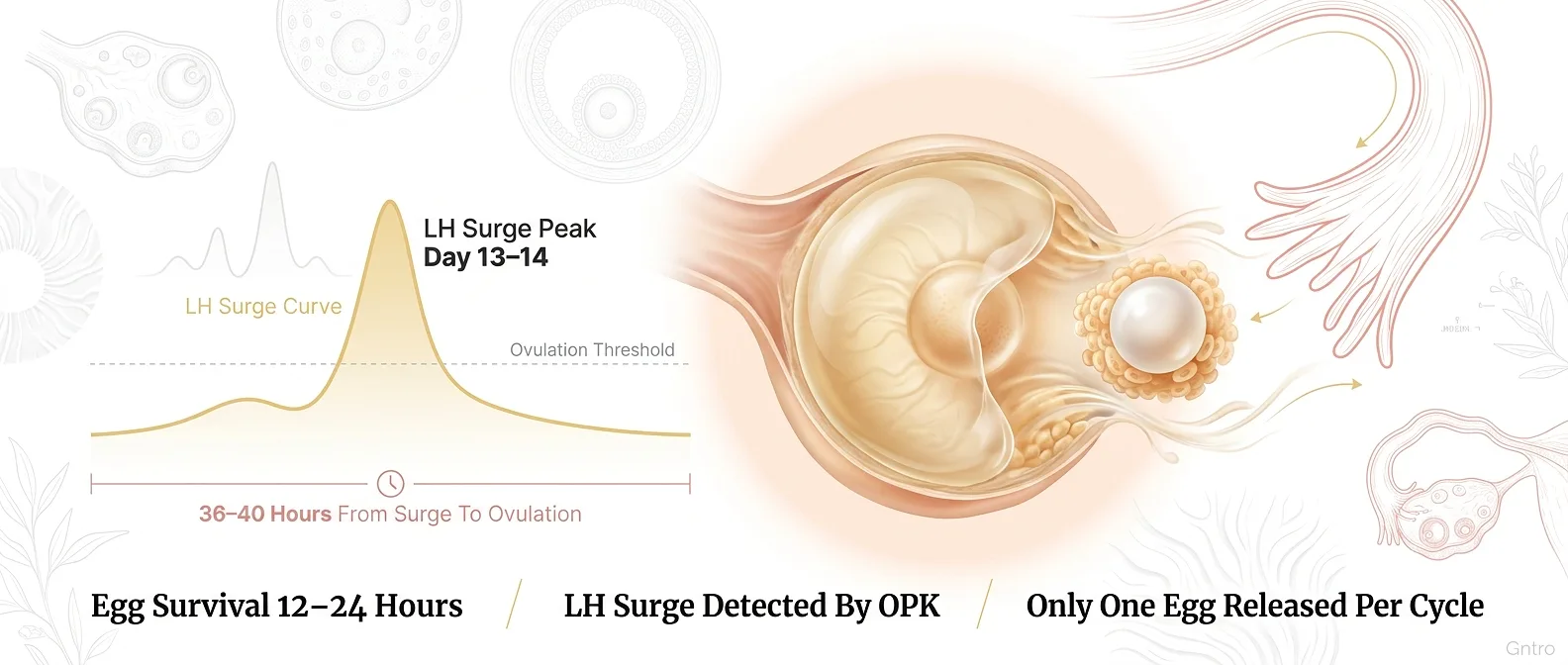
- Day 13-14: Rising oestradiol levels trigger the pituitary gland to release a sharp spike of LH – the LH surge.
This LH surge is the biological trigger for ovulation. It is also what commercial ovulation predictor kits (OPKs) detect in your urine.
Key point: The follicular phase varies in length between women and from cycle to cycle. This is why ovulation does not always happen on day 14 – it depends entirely on when your LH surge occurs.
Phase 2: The LH Surge and the Moment of Ovulation
Approximately 36-40 hours after the LH surge begins (and 10-12 hours after it peaks), ovulation occurs.
Here is the exact sequence:
- The LH surge triggers a cascade of enzymatic activity within the dominant follicle.
- The follicle wall weakens and eventually ruptures – a process called follicular rupture.
- The mature secondary oocyte is released into the peritoneal (abdominal) cavity.
- The fimbriae – finger-like projections at the end of the fallopian tube – sweep the egg up and into the tube. This is a remarkably precise process, given that the ovary and tube are not physically connected.
- The egg begins its journey down the fallopian tube toward the uterus.
According to NIH research on ovulation physiology, the released egg survives for only 12 to 24 hours. This is your fertilisation window. If no sperm fertilises the egg within this period, the egg disintegrates and is absorbed.
After ovulation, the ruptured follicle transforms into a temporary endocrine structure called the corpus luteum, which produces progesterone. Progesterone thickens the uterine lining and prepares it for implantation.
Phase 3: The Fertilisation Window – Sperm’s Race Against Time
While the egg’s window is just 12-24 hours, sperm are considerably more resilient. Healthy sperm can survive inside the female reproductive tract for up to 5 days – which is why your fertile window is wider than you might think.
Your fertile window typically spans 6 days:
| Day Relative to Ovulation | Chance of Conception |
|---|---|
| 5 days before ovulation | ~5% |
| 4 days before ovulation | ~11% |
| 3 days before ovulation | ~15% |
| 2 days before ovulation | ~20% |
| 1 day before ovulation | ~26% |
| Day of ovulation | ~33% |
This is why many fertility experts recommend beginning intercourse 2-3 days before expected ovulation, rather than only on the day itself.
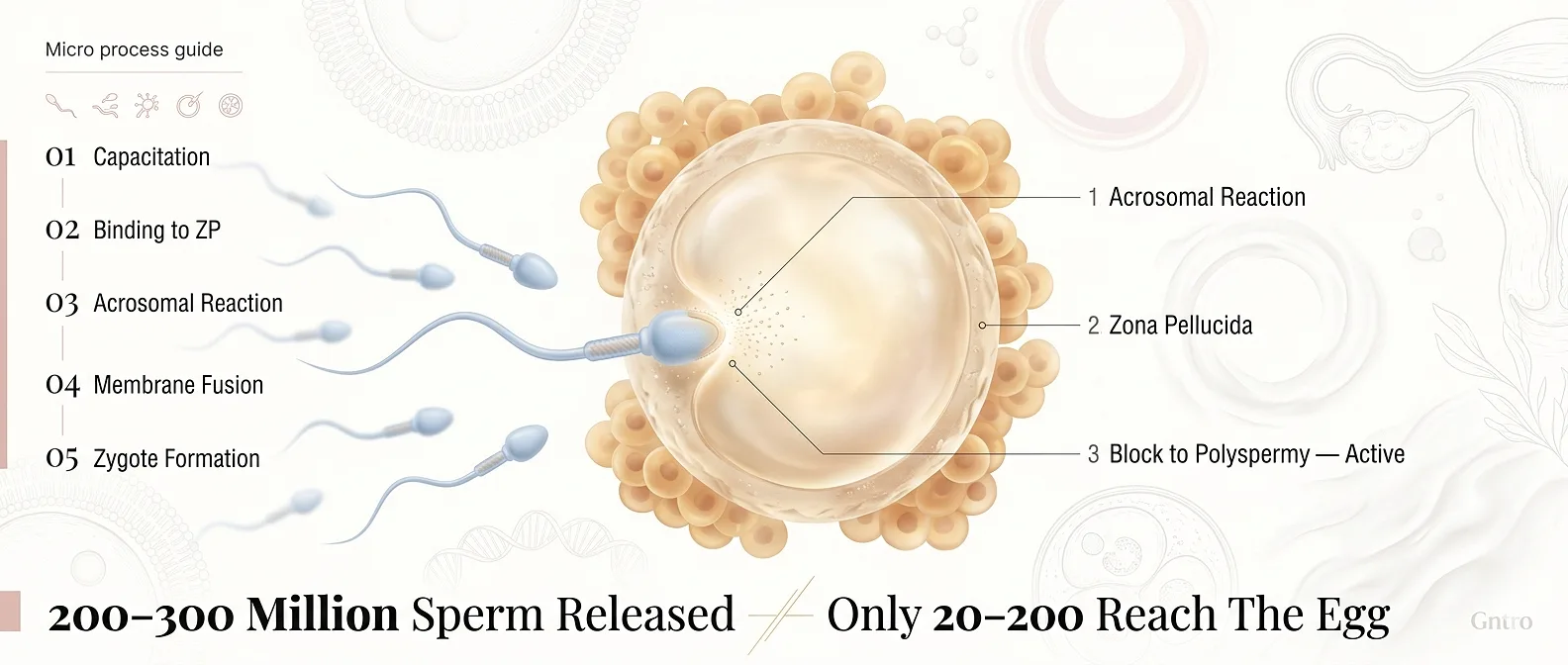
After ejaculation, sperm undergo a process called capacitation within the female reproductive tract. This is a physiological change that makes them capable of fertilising an egg – they become hyperactivated, swimming more vigorously in a whip-like pattern.
Of the approximately 200-300 million sperm in a single ejaculate, only a few hundred typically reach the fallopian tube, and only 20-200 actually reach the egg. This is not random: the female reproductive tract actively selects for the highest-quality sperm.
Phase 4: Fertilisation Step by Step
Fertilisation itself is a multi-stage molecular event. Here is exactly what happens:
Step 1: Sperm Meets Egg
The strongest sperm arrive at the ampullary region of the fallopian tube, where the egg awaits. The egg is surrounded by layers of cells:
- The cumulus oophorus (a cloud of granulosa cells)
- The zona pellucida (ZP) – a glycoprotein shell
Step 2: Acrosomal Reaction
When a sperm contacts the zona pellucida, the acrosomal reaction is triggered. The tip of the sperm (the acrosome) releases digestive enzymes – primarily acrosin and hyaluronidase – that dissolve a path through the zona pellucida.
Step 3: Cortical Reaction and Block to Polyspermy
The instant one sperm penetrates the zona pellucida and contacts the egg’s plasma membrane, the egg triggers the cortical reaction: it releases enzymes that rapidly harden the zona pellucida, preventing any other sperm from entering. This is the block to polyspermy – a critical quality-control mechanism.
Step 4: Fusion of Genetic Material
The sperm’s head enters the egg cytoplasm. Both the sperm’s nucleus and the egg’s nucleus (which resumes its second meiotic division upon sperm entry) release their chromosomes. These combine to form the full diploid genome of the zygote – a completely unique individual.
Step 5: Zygote Formation
Within 12-24 hours of fertilisation, the zygote undergoes its first mitotic division, creating a 2-cell embryo. This is the beginning of cleavage.
According to NIH’s embryology research on fertilisation, this entire fertilisation process is complete within 24 hours of the sperm reaching the egg.
Phase 5: Implantation – When Pregnancy Truly Begins
After fertilisation, the journey is far from over. The embryo must travel from the fallopian tube to the uterus, develop further, and successfully implant in the uterine lining.
Here is the timeline:
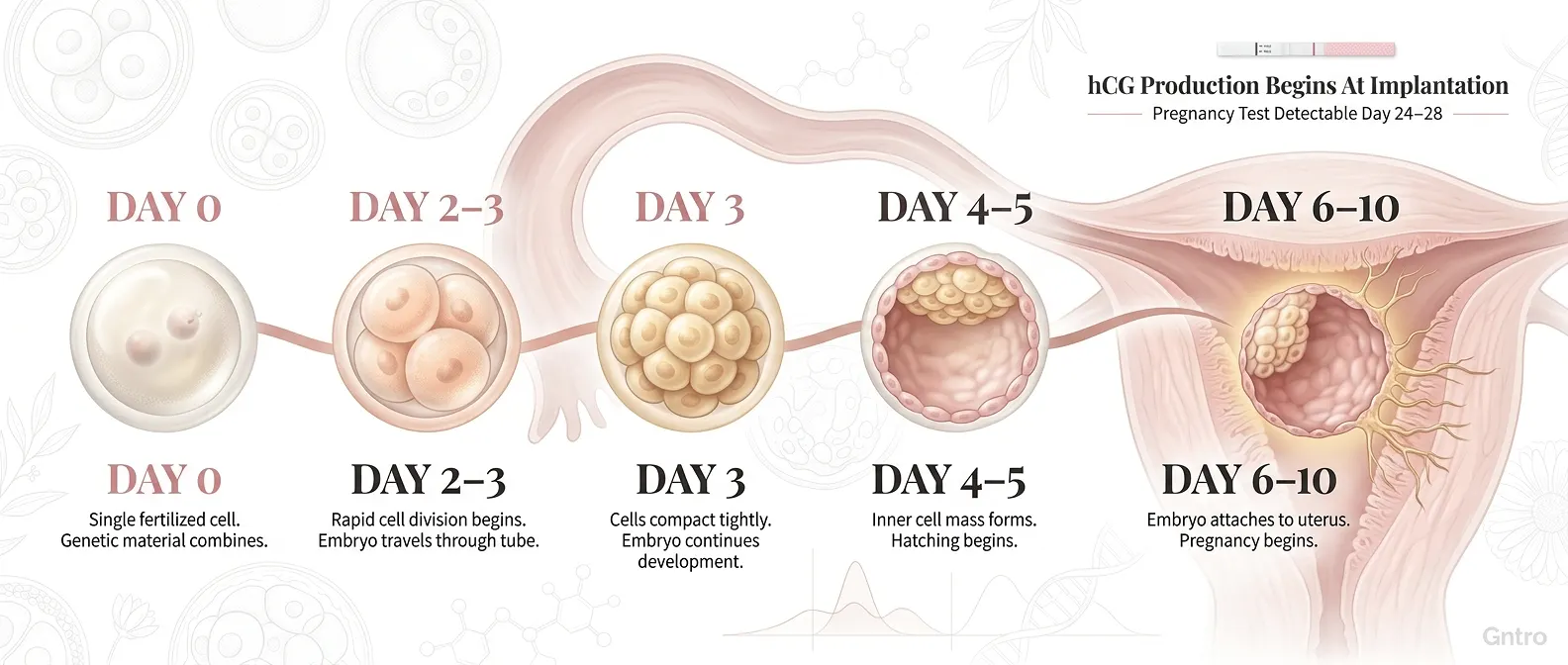
Day 1-3 Post-Fertilisation: Cleavage and Morula Stage
The zygote undergoes rapid cell divisions (cleavage) as it travels toward the uterus. By Day 3, it has become a morula – a compact ball of 16 cells. Crucially, the overall size does not increase; the cells simply get smaller with each division.
Day 4-5: Blastocyst Formation
The morula develops a fluid-filled cavity and becomes a blastocyst. The blastocyst has two distinct cell populations:
- Inner cell mass (ICM): Will become the embryo itself.
- Trophoblast cells: Will form the placenta and membranes.
The blastocyst also sheds its zona pellucida in a process called hatching – this is necessary for implantation.
Day 6-10: Implantation
The blastocyst arrives in the uterine cavity. It makes contact with the receptive endometrium (uterine lining) and implantation occurs in three stages:
- Apposition: The blastocyst loosely positions itself against the endometrial surface.
- Adhesion: Trophoblast cells form a firmer attachment to the endometrial epithelium.
- Invasion: Trophoblast cells invade the endometrial stroma, anchoring the embryo and beginning placental formation.
As the trophoblast cells invade, they begin producing human chorionic gonadotropin (hCG) – the hormone detected by home pregnancy tests. HCG signals the corpus luteum to keep producing progesterone, preventing menstruation and maintaining the pregnancy.
This is the moment a pregnancy is clinically established.
How to Recognise Ovulation: Signs Every Indian Woman Should Know
One of the most practical steps you can take is learning to recognise your body’s natural ovulation signals. These signs do not require expensive technology – many can be tracked with simple observation.
Primary Signs of Ovulation
1. Changes in Cervical Mucus (Most Reliable)
In the days leading up to ovulation, your cervical mucus changes noticeably:
- Early cycle: Dry or sticky, opaque white
- Approaching ovulation: Creamy, white, lotion-like
- At peak fertility: Clear, slippery, stretchy – resembling raw egg whites (sometimes called “egg-white cervical mucus” or EWCM)
This egg-white consistency is the single most reliable sign that ovulation is imminent. The mucus creates an environment that supports sperm survival and guides sperm toward the egg.
2. Basal Body Temperature (BBT) Rise
Your resting body temperature rises by approximately 0.2-0.5°C after ovulation occurs, due to increased progesterone. Tracking BBT daily with a basal thermometer (measured first thing in the morning before getting out of bed) can help you confirm ovulation has occurred – though it cannot predict it in advance.
3. LH Surge (via Ovulation Predictor Kits)
Commercially available OPKs detect the LH surge in urine, typically 24-36 hours before ovulation. This is the most accurate non-invasive predictor. Testing twice daily (morning and early evening) increases accuracy.
Secondary Signs of Ovulation
- Mittelschmerz: Mild one-sided pelvic pain or cramping lasting minutes to a few hours, caused by follicular rupture.
- Breast tenderness: Due to rising oestrogen and progesterone.
- Increased libido: A natural biological drive to conceive at peak fertility.
- Abdominal bloating: Light bloating around the mid-cycle.
- Heightened sense of smell: Some women report increased sensitivity to odours.
- Cervical changes: The cervix becomes higher, softer, and more open (SHOW: Soft, High, Open, Wet).
The Fertile Window: A Practical Guide for Indian Women Trying to Conceive
Understanding the fertile window is central to grasping what is ovulation and conception in practical terms. Here is how to identify and use yours:
Step-by-Step: Tracking Your Fertile Window
1st Step: On Day 1 of your period, start tracking.
2nd Step: Each morning before rising, take your basal body temperature with a basal (not standard) thermometer and log it.
3rd Step: Each evening, check your cervical mucus and note its consistency.
4th Step: From Day 10 of your cycle, begin using an OPK each morning and afternoon.
5th Step: When you observe egg-white cervical mucus AND your OPK turns positive, you are in your most fertile window.
6th Step: Have intercourse on the day of a positive OPK, the day after, and ideally the day before as well.
7th Step: After your BBT rises and stays elevated for 3+ days, ovulation has occurred and your fertile window has closed for that cycle.
For Indian Women With Irregular Cycles
Many Indian women experience cycle irregularities due to PCOS, stress, or dietary factors. If your cycle varies by more than 7 days month to month:
- Do not rely solely on day-counting or standard calculators.
- Prioritise cervical mucus observation and OPK testing.
- Consider consulting a fertility specialist if your cycles are consistently irregular.
Common Mistakes Indian Women Make When Trying to Conceive
Even motivated, well-informed women make avoidable errors. Here are the most common mistakes – and how to correct them:
Mistake 1: Only Timing Intercourse on the Day of Ovulation
The error: Waiting until the OPK turns positive and only then having intercourse.
Why it’s a problem: The egg survives only 12-24 hours. If timing is slightly off, or if sperm quality is suboptimal, conception may not occur.
The fix: Begin having intercourse 2-3 days before expected ovulation to ensure sperm are already in the fallopian tube when the egg arrives.
Mistake 2: Ignoring Lifestyle Factors That Affect Ovulation
The error: Focusing only on timing while neglecting nutrition, sleep, and stress management.
Why it’s a problem: Chronic stress elevates cortisol, which directly suppresses GnRH secretion and can delay or suppress ovulation entirely. Poor diet and low body weight similarly disrupt the HPO axis.
The fix: Address stress, maintain a healthy BMI, and ensure adequate micronutrient intake – particularly folate, iron, vitamin D, and zinc.
Mistake 3: Assuming a 28-Day Cycle
The error: Using apps or generic calendars that assume ovulation always falls on Day 14.
Why it’s a problem: Fewer than 15% of women actually ovulate on Day 14. Indian women, with higher rates of PCOS and thyroid disorders, are especially likely to ovulate later or irregularly.
The fix: Track your own data for at least 2-3 cycles before predicting ovulation dates.
Mistake 4: Not Accounting for Sperm Health
The error: Focusing only on the woman’s cycle while overlooking male factor fertility.
Why it’s a problem: Approximately 40-50% of all infertility cases involve a male factor. Sperm quality directly affects whether fertilisation can occur.
The fix: Both partners should pursue preconception health optimisation – not just the woman.
Mistake 5: Excessive Intercourse (Oversampling)
The error: Having intercourse multiple times daily throughout the entire fertile window, thinking more is better.
Why it’s a problem: Very frequent ejaculation can temporarily reduce sperm concentration and motility.
The fix: Aim for intercourse once every 24-48 hours during your fertile window for optimal sperm quality and timing.
Expert Tips to Support Ovulation and Natural Conception
Supporting healthy ovulation requires a whole-body approach. These evidence-informed strategies are particularly relevant for Indian women:
Nutrition for Ovulatory Health
- Folate-rich foods: Leafy greens such as methi (fenugreek), spinach, and curry leaves support healthy egg development and reduce neural tube defect risk. Start supplementing with 400-800mcg of folic acid before conception.
- Iron: Dal (lentils), kidney beans, and fortified foods support adequate blood supply to the reproductive organs.
- Antioxidants: Turmeric, amla, and berries protect egg quality from oxidative damage.
- Healthy fats: Include ghee (in moderation), nuts, seeds, and coconut – essential fat-soluble vitamins A, D, E, and K are vital for hormonal health.
- Limit refined carbohydrates: High glycaemic index foods spike insulin, which elevates androgens and disrupts ovulation – particularly problematic for women with PCOS.
Lifestyle Adjustments
- Maintain a healthy BMI (18.5-24.9). Both underweight and overweight status disrupts the HPO axis.
- Aim for 7-8 hours of quality sleep each night. Growth hormone and LH secretion are highest during deep sleep.
- Manage stress actively through yoga, pranayama (breathwork), or meditation – practices deeply embedded in Indian wellness culture and scientifically validated for reducing cortisol.
- Avoid smoking and alcohol – both directly impair egg quality and hormonal signalling.
Supplements to Discuss With Your Doctor
- Coenzyme Q10 (CoQ10): Supports mitochondrial function in oocytes – particularly useful for women over 32.
- Vitamin D: Deficiency is extremely common in India and is linked to irregular ovulation and reduced fertility.
- Myo-inositol: Especially beneficial for women with PCOS, as it improves insulin sensitivity and restores ovulatory function.
- Omega-3 fatty acids: Support anti-inflammatory prostaglandin pathways and improve endometrial receptivity.
Reminder: Always consult your gynaecologist or fertility specialist before starting any supplement protocol.
Ovulation, Fertilisation, and Implantation: Quick Reference Summar
What is ovulation and conception: a quick summary
- Ovulation: The release of a mature egg from the ovary, triggered by an LH surge, occurring approximately mid-cycle.
- Fertilisation: The fusion of a sperm cell and egg in the fallopian tube, forming a zygote.
- Implantation: The embedding of the blastocyst into the uterine lining, typically 6-10 days after fertilisation.
- Key window: The fertile window spans approximately 6 days per cycle – the 5 days before ovulation and the day of ovulation itself.
- Pregnancy confirmed: When the implanted embryo produces sufficient hCG to be detected by a pregnancy test (approximately 12-14 days after ovulation).
Comparison Table: Natural Conception vs. Assisted Reproduction
| Factor | Natural Conception | IVF / Assisted Reproduction |
|---|---|---|
| Ovulation required | Yes – spontaneous | No – stimulated with medication |
| Fertilisation location | Fallopian tube | Laboratory |
| Implantation | Natural | Embryo transfer into uterus |
| Monthly success rate (under 35) | 20-25% | 40-50% per transfer |
| Cost | Low | High |
| Invasiveness | None | Moderate to high |
| Hormonal intervention | None | Significant |
| Best suited for | Couples without identified fertility barriers | Couples with blocked tubes, severe MFI, or failed natural conception |
Frequently Asked Questions
Q1: What is ovulation and conception in simple terms?
Ovulation is when your ovary releases a mature egg once per menstrual cycle. Conception is when that egg is fertilised by a sperm cell, creating an embryo. Together, ovulation and conception are the two essential steps that must occur for pregnancy to begin.
Q2: How long does ovulation last?
Ovulation itself – the actual release of the egg – happens within a few minutes. However, the egg remains viable and fertilisable for 12 to 24 hours after release. The fertile window, which includes sperm survival time, spans approximately 6 days per cycle.
Q3: Can I get pregnant without knowing I ovulated?
Yes. Many women, particularly those with irregular cycles or PCOS, may ovulate without obvious symptoms. This is why tracking cervical mucus and using OPKs is more reliable than relying solely on perceived symptoms.
Q4: What are the signs that ovulation has occurred?
After ovulation, you may notice: a sustained rise in BBT of 0.2-0.5°C, a shift from egg-white cervical mucus to thicker, sticky discharge, disappearance of OPK positivity, and occasionally mild pelvic cramping (mittelschmerz). The BBT rise is the most reliable confirmation that ovulation has occurred.
Q5: How soon after conception does a pregnancy test turn positive?
A home urine pregnancy test can typically detect hCG levels 10-14 days after fertilisation (i.e., around the time your next period would be due). Blood tests (beta-hCG) can detect pregnancy earlier – sometimes as early as 7-10 days post-fertilisation.
Q6: Does stress affect ovulation and conception?
Yes, significantly. Elevated cortisol levels – a direct result of chronic stress – suppress GnRH secretion from the hypothalamus, which in turn reduces FSH and LH output. This can delay ovulation, cause anovulatory cycles, or produce a shortened, inadequate luteal phase. Managing stress is not optional: it is a core fertility strategy.
Q7: Is ovulation painful?
Some women feel mittelschmerz – a mild, one-sided pain or ache in the lower abdomen at the time of ovulation. It may last from a few minutes to several hours. It is typically not severe. However, intense ovulation pain warrants medical evaluation to rule out conditions like ovarian cysts or endometriosis.
Q8: What is the difference between ovulation and conception for someone with PCOS?
Women with PCOS often experience oligo-ovulation (infrequent ovulation) or anovulation (absent ovulation), because elevated androgens and insulin resistance disrupt the LH-FSH ratio. This means conception is harder to achieve naturally. However, with appropriate lifestyle changes, dietary modifications, and targeted supplementation (such as myo-inositol), many women with PCOS do restore regular ovulation and conceive naturally.
Understanding Ovulation and Conception Is Your Most Powerful Fertility Tool
Understanding what is ovulation and conception, at a detailed physiological level, gives you something no supplement or app alone can provide: genuine insight into your own reproductive biology. You now know that ovulation is not simply “releasing an egg” – it is the culmination of a precise 13-day hormonal cascade. You understand that fertilisation is not guaranteed; it is a competitive, molecular event with multiple biological safeguards. And you recognise that implantation is the true beginning of pregnancy, not the moment of intercourse.
For Indian women, navigating this journey comes with additional nuances: higher prevalence of PCOS and thyroid disorders, dietary considerations unique to Indian food culture, and the psychological pressures of family expectations around conception. None of these barriers are insurmountable, and they are significantly more manageable when you are well-informed.
This knowledge is your starting point. The next step is personalised guidance.
If you are ready to move from understanding your cycle to actively optimizing it for conception, explore Gntro’s science-backed preconception support programmes and get the exact answers for How to get pregnant – designed specifically to help women like you conceive naturally, with confidence and clinical support behind every step.