PCOS (Polycystic Ovary Syndrome) does not always prevent ovulation completely; rather, it causes oligo-ovulation – a pattern of infrequent, unpredictable, or delayed ovulation rather than a total absence of ovulatory cycles. In clinical terms, PCOS disrupts the hypothalamic-pituitary-ovarian (HPO) axis, elevating LH:FSH ratios and driving androgen excess, which impairs follicular maturation and suppresses the mid-cycle LH surge required for ovulation. This means many women with PCOS do ovulate occasionally, but the timing remains erratic and difficult to predict without tracking.
If you have been diagnosed with PCOS and are wondering whether you can still conceive, you are far from alone. Millions of Indian women live with this condition, and a great deal of confusion surrounds what PCOS actually does to the monthly cycle. This article breaks down exactly what happens to ovulation when you have PCOS, how to detect those elusive ovulatory windows, and what steps Indian women can take to support their fertility naturally.
For women navigating this journey, understanding your hormones and cycle patterns is the first step. If you are looking for personalised support on how to get pregnant with PCOS or other hormonal challenges, Gntro offers science-backed guidance tailored to the Indian context.
What Exactly is PCOS and Why Does It Affect Ovulation?
PCOS is one of the most common hormonal disorders affecting women of reproductive age. In India, studies estimate that anywhere between 9% to 22% of women have PCOS, making it far more prevalent here than in many Western populations. Yet it remains widely misunderstood, both by women who have it and even by some healthcare providers.
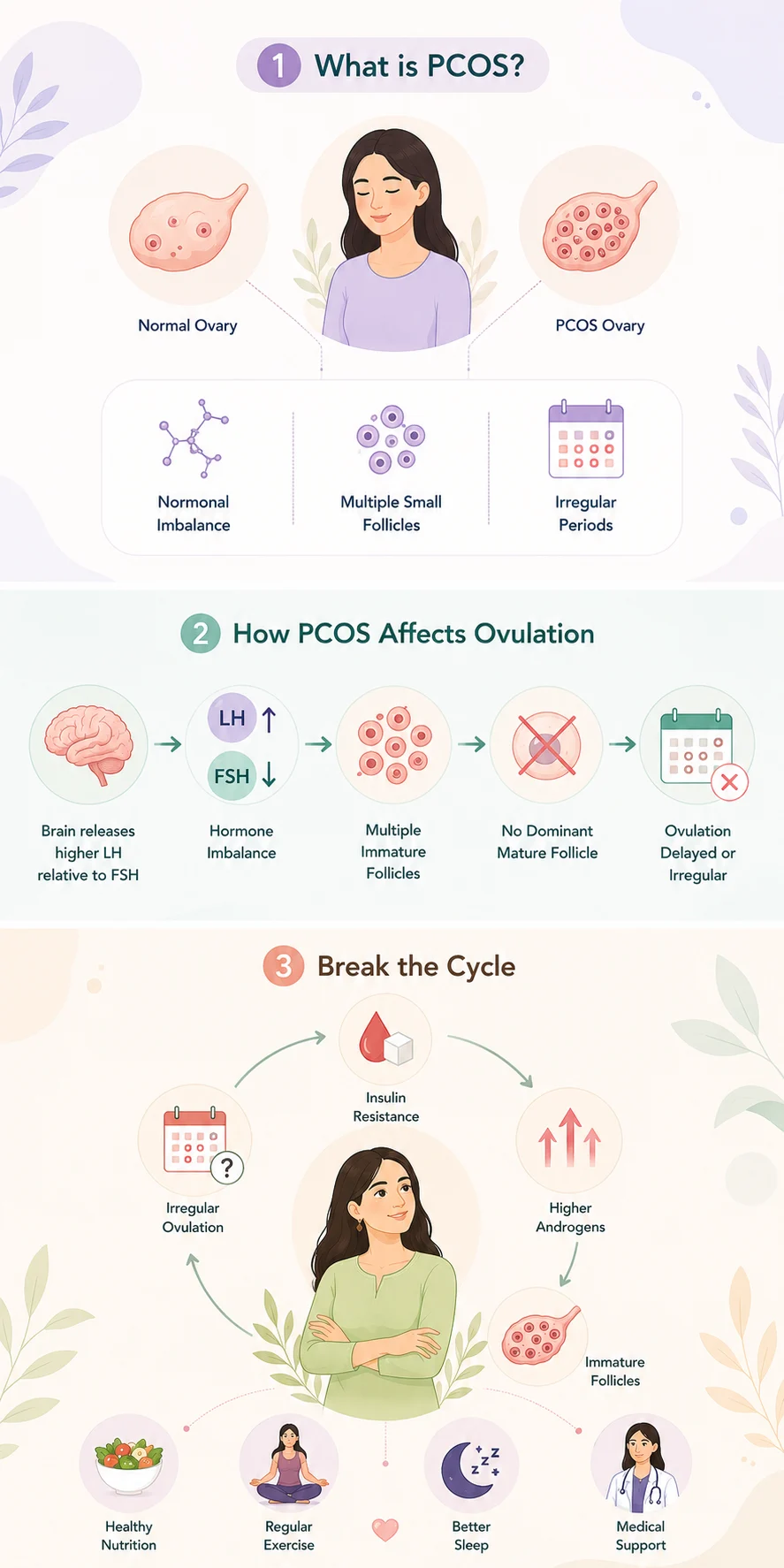
At its core, PCOS is a condition characterised by:
- Elevated androgens (male hormones like testosterone) circulating in the blood
- Polycystic ovaries – ovaries that contain multiple small follicles that do not mature fully
- Irregular or absent menstrual cycles caused by disrupted ovulation
The reason PCOS affects ovulation so directly comes down to hormonal imbalance. During a normal cycle, the follicle-stimulating hormone (FSH) encourages one follicle to mature each month. Once mature, a surge of luteinising hormone (LH) triggers ovulation. In women with PCOS, this sequence gets disrupted.
Here is what typically happens:
- The brain releases higher-than-normal levels of LH relative to FSH.
- This imbalance prevents follicles from fully maturing.
- Multiple small, immature follicles accumulate on the ovaries (the “cysts” in PCOS, though they are not true cysts).
- Without a dominant mature follicle, the LH surge does not fire correctly.
- Ovulation is delayed, skipped, or irregular.
Additionally, many women with PCOS have insulin resistance, which further drives androgen production from the ovaries. Higher androgens, in turn, further suppress normal follicular development – creating a vicious cycle.
To understand this in greater depth, it helps to learn what ovulation is and what happens step by step during a normal cycle, so you can spot when your body deviates from that pattern.
Does PCOS Prevent Ovulation Completely? The Honest Answer
This is the question most women ask first, and the answer is nuanced: No, PCOS does not prevent ovulation completely for most women.
What PCOS does is make ovulation unpredictable and infrequent. Medically, this is called:
- Oligoovulation – ovulating fewer than eight times per year
- Anovulation – not ovulating at all in a given cycle
The majority of women with PCOS fall into the oligoovulation category. This means they do ovulate, but perhaps once every 35 to 90 days instead of every 28 days. Some cycles they ovulate, others they do not – and there is no reliable calendar pattern to predict which is which.
A smaller subset of women with severe PCOS experience near-complete anovulation, where ovulation rarely or never occurs without medical intervention. However, this is not the norm.
Key Takeaway
| Ovulation Pattern | What It Means for PCOS | How Common? |
|---|---|---|
| Regular ovulation (every 21-35 days) | PCOS may be mild; hormones relatively balanced | Less common |
| Oligoovulation (8 or fewer cycles/year) | Typical PCOS pattern | Most common |
| Anovulation (no ovulation) | Severe hormonal disruption; may need medical help | Less common |
| Sporadic ovulation | Can ovulate in some cycles, not others | Very common |
This matters enormously for conception planning. If you ovulate occasionally and unpredictably, you can get pregnant naturally – but you need to track your cycle carefully to catch that window.
How PCOS Disrupts the Menstrual Cycle in Indian Women: Additional Factors
While PCOS physiology is universal, several factors specific to the Indian context can worsen its impact on ovulation.
- Diet High in Refined Carbohydrates Traditional Indian diets, particularly in urban settings, often include large amounts of refined grains – white rice, maida-based bread, and sugary snacks. These foods cause rapid spikes in blood sugar and insulin. Since insulin resistance is a major driver of PCOS, a high-glycaemic diet can worsen the hormonal imbalance and further suppress ovulation. Switching to a fertility-supportive diet plan rich in complex carbohydrates, healthy fats, and anti-inflammatory foods can make a measurable difference to ovulation frequency in women with PCOS.
- Vitamin D Deficiency India has surprisingly high rates of Vitamin D deficiency despite abundant sunshine. Vitamin D plays a direct role in insulin sensitivity and ovarian function. Low Vitamin D levels are associated with worse PCOS outcomes, including less regular ovulation.
- Chronic Stress Psychological stress elevates cortisol, which disrupts the HPO axis further. Given the pressures many Indian women face – balancing family expectations, career, and societal norms around marriage and motherhood – chronic stress is an underappreciated factor that worsens PCOS-related cycle disruption.
- Lack of Awareness and Delayed Diagnosis Many Indian women are diagnosed with PCOS only when they struggle to conceive. By this point, years of unmanaged insulin resistance and inflammation may have compounded the hormonal imbalance. Early identification and lifestyle intervention can significantly preserve ovulatory function.
Signs That You Might Still Be Ovulating With PCOS
Even with PCOS, your body often gives signs when ovulation does occur. Learning to recognise these can be genuinely empowering.
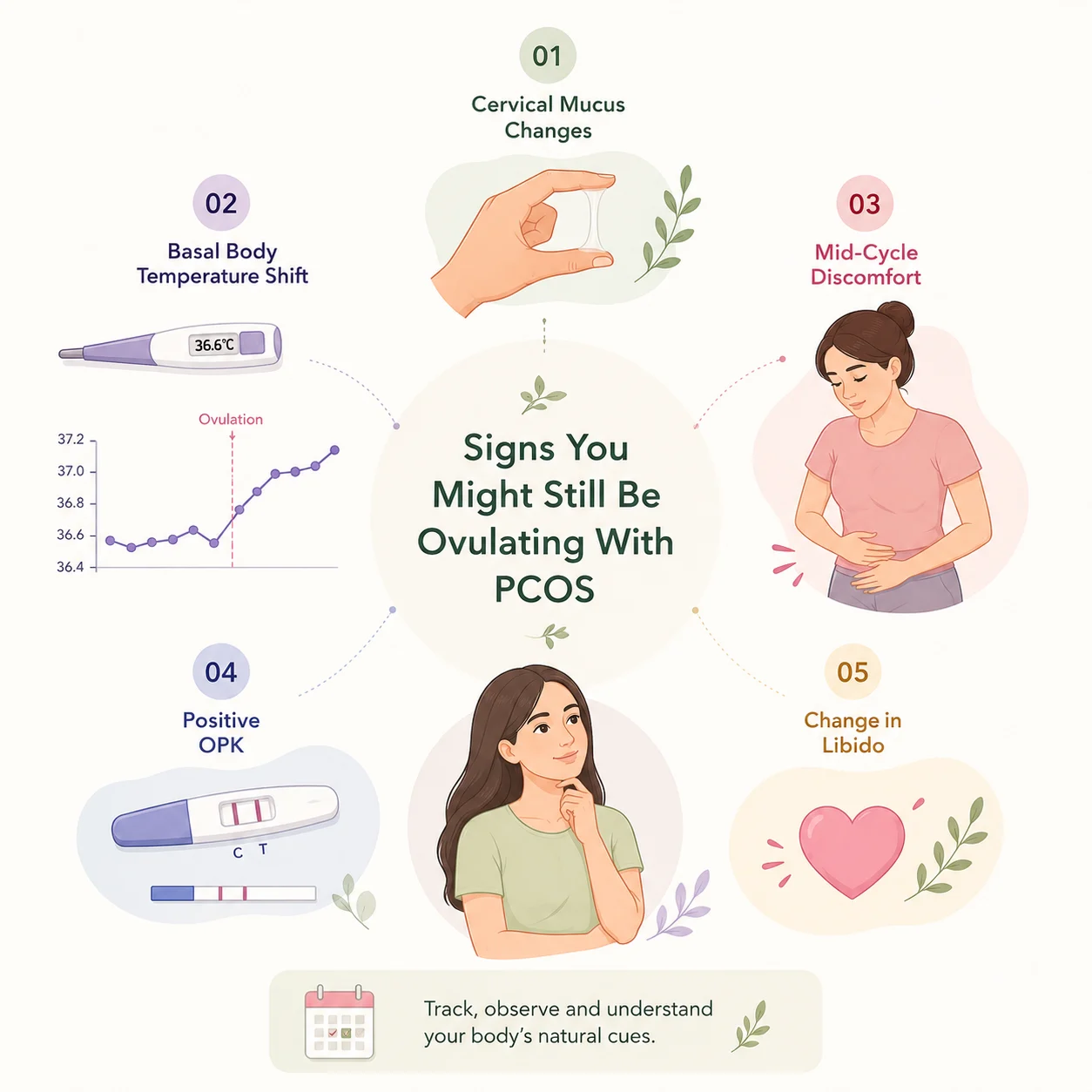
- Cervical Mucus Changes In the days approaching ovulation, oestrogen rises and causes cervical mucus to become clear, slippery, and stretchy, similar to raw egg white. Women with PCOS should watch for this change even if periods are irregular, as it signals that a follicle is maturing and ovulation may be near.
- Basal Body Temperature (BBT) Shift After ovulation, progesterone causes a slight but consistent rise in resting body temperature (typically $0.2-0.5^{\circ}C$). Tracking BBT every morning with a sensitive thermometer before getting out of bed can confirm whether ovulation has occurred. With PCOS, you may not see this rise every cycle, but when it appears, it confirms ovulation took place.
- Positive Ovulation Predictor Kit (OPK) OPKs detect the LH surge that precedes ovulation. However, women with PCOS can have elevated baseline LH levels, which sometimes causes false positives. Using OPKs in conjunction with BBT tracking and cervical mucus observation gives a more reliable picture.
- Change in Libido Many women notice a natural increase in sexual desire around ovulation, driven by the mid-cycle oestrogen surge. This is a subtle but real hormonal cue.
- Mid-Cycle Pelvic Discomfort Some women feel a mild ache or twinge on one side of the lower abdomen during ovulation – called mittelschmerz. This is not a universal sign, but if you experience it, it is worth noting in your cycle diary.
How to Track Ovulation Effectively When You Have PCOS
Because PCOS makes the standard 28-day calendar method unreliable, you need a more evidence-based approach.
Step-by-Step Cycle Tracking for PCOs
- Step 1: Start a dedicated cycle diary or app Record the date your period starts each month. Note any symptoms: spotting, pelvic pain, changes in energy, mood, or libido.
- Step 2: Track basal body temperature daily Take your temperature every morning at the same time before rising. Use a thermometer calibrated to two decimal places. Note the reading and look for the sustained rise that confirms ovulation.
- Step 3: Monitor cervical mucus Check your cervical mucus every day and record its quality – dry, creamy, watery, or egg-white consistency. The egg-white phase typically occurs 1-2 days before ovulation.
- Step 4: Use OPKs strategically Begin testing around day 10 of your cycle if your cycles are 35 days or shorter. If your cycles run longer, start testing around day 14-16. Test twice daily (morning and early afternoon) for greatest accuracy.
- Step 5: Combine all three signals A confirmed ovulation requires: a positive OPK (rising LH), egg-white cervical mucus, and a post-ovulatory BBT rise. Waiting for all three aligns you for the most fertile window.
- Step 6: Note when intercourse would be most timely The fertile window spans approximately 5 days before ovulation to the day of ovulation itself. Sperm can survive up to 5 days in fertile cervical mucus, so timing intercourse in this period maximises the chance of conception. For detailed guidance on this, review expert advice on the best time to have intercourse to conceive.
Can Lifestyle Changes Restore Ovulation in PCOS?
Yes – and this is one of the most encouraging aspects of managing PCOS. Because insulin resistance is a central driver for many women, targeted lifestyle changes can genuinely restore more regular ovulation without medication.
- Weight Management Research published in journals including Human Reproduction consistently shows that even a 5-10% reduction in body weight can restore ovulatory cycles in overweight women with PCOS. However, not all Indian women with PCOS are overweight. Lean PCOS is also common in India, and these women benefit from different strategies focused more on reducing inflammation and stress.
- Low-Glycaemic Diet Reducing refined carbohydrates and replacing them with complex carbs, pulses, vegetables, and healthy fats lowers insulin levels. This, in turn, reduces ovarian androgen production and allows follicles to mature more normally. Incorporating Indian foods that support fertility – like methi (fenugreek), amla, sesame seeds, and dals – is both practical and effective. For women trying to conceive, folic acid is also critical. Indian food sources like leafy greens, lentils, and fortified cereals are key, and you can find a practical breakdown of the best Indian food sources of folic acid for women trying to conceive.
- Exercise Both aerobic exercise and resistance training improve insulin sensitivity and reduce circulating androgens. The key is consistency rather than intensity. Even 30 minutes of brisk walking five days per week produces measurable hormonal improvements in women with PCOS, according to the American College of Obstetricians and Gynecologists (ACOG).
- Stress Reduction Yoga, meditation, and adequate sleep all reduce cortisol and support healthy HPO axis function. Several Indian studies have specifically looked at yoga’s effect on PCOS and found improvements in menstrual regularity, hormonal profiles, and ovulation frequency.
Supplements With Evidence
The following supplements have research supporting their role in PCOS management:
- Myo-inositol (and D-chiro-inositol): Improves insulin signalling in ovarian cells and is one of the most studied natural interventions for PCOS. Multiple randomised controlled trials show improved ovulation rates.
- N-Acetyl Cysteine (NAC): An antioxidant that improves insulin sensitivity and may trigger ovulation in anovulatory PCOS.
- Vitamin D: Addresses deficiency and supports follicular development.
- Magnesium: Supports insulin receptor function and reduces androgens.
- Always discuss supplements with your doctor before starting them, especially if you are trying to conceive.

When Does PCOS Require Medical Treatment for Ovulation?
Lifestyle changes are the first line of treatment, but they are not always sufficient – particularly when a woman is actively trying to conceive and has not achieved pregnancy after 6-12 months of trying.
Medical options your gynaecologist or reproductive endocrinologist may recommend include:
- Letrozole (First-Line Treatment) Letrozole, an aromatase inhibitor, is now the preferred first-line ovulation induction agent for PCOS in most international guidelines, including those from the ESHRE (European Society of Human Reproduction and Embryology). It works by temporarily lowering oestrogen levels, prompting the brain to release more FSH, which drives follicular development and ovulation.
- Clomiphene Citrate (Clomid) For years, Clomid was the standard treatment for anovulatory PCOS. It works by blocking oestrogen receptors in the hypothalamus, increasing FSH release. However, Letrozole now has a stronger evidence base for PCOS specifically, and is less likely to cause the cervical mucus thinning associated with Clomid.
- Metformin An insulin-sensitising medication originally developed for type 2 diabetes, Metformin improves insulin resistance and can restore ovulation in many women with PCOS, particularly those with elevated fasting insulin levels. It is often used in combination with Letrozole.
- Gonadotropins Injectable FSH (gonadotropins) can directly stimulate follicular development when oral medications have not worked. However, they carry a higher risk of multiple pregnancies and require close monitoring.
- Laparoscopic Ovarian Drilling (LOD) This surgical procedure uses heat or laser to destroy small portions of ovarian tissue that produce excess androgens. It can restore ovulation in some women who have not responded to medication, though it is used less commonly now given the effectiveness of medical treatments.
Common Myths About PCOS and Ovulation Indian Women Should Stop Believing
- Myth 1: “If I Have PCOS, I Can Never Get Pregnant Naturally” False. Many women with PCOS conceive naturally, particularly when they track ovulation carefully and address the underlying hormonal drivers through lifestyle and, if needed, medication.
- Myth 2: “Irregular Periods Mean I Am Not Ovulating at All” Not necessarily. Irregular periods often reflect irregular ovulation, not complete anovulation. You may be ovulating every 45 or 60 days rather than every 28.
- Myth 3: “Hormonal Contraceptives Cure PCOS” Oral contraceptive pills regulate the cycle and reduce androgens while you take them, but they do not address the underlying insulin resistance or hormonal drivers. After stopping the pill, PCOS symptoms and irregular ovulation typically return.
- Myth 4: “Thin Women Do Not Get PCOS” Lean PCOS is well-documented and is particularly prevalent in South Asian women. Body weight alone does not determine PCOS risk or severity.
- Myth 5: “Once I Have One Child With PCOS, My Cycle Will Normalise” Pregnancy does not cure PCOS. Some women notice improved cycle regularity postpartum, but many do not. Ongoing management is important.
Comparison: Normal Ovulation vs. PCOS Ovulation
| Feature | Normal Ovulatory Cycle | PCOS Ovulation Pattern |
|---|---|---|
| Cycle length | 21-35 days | 35-90+ days (or longer) |
| Ovulation predictability | Consistent, mid-cycle | Irregular, unpredictable |
| LH surge | Clear and brief | May be elevated chronically or absent |
| Cervical mucus changes | Distinct egg-white phase | May be present but timing unclear |
| BBT rise | Reliable post-ovulatory shift | Present when ovulation occurs |
| Progesterone in second half | Rises normally | May be low if ovulation was weak |
| OPK reliability | Highly reliable | Can show false positives |
What to Tell Your Doctor: Getting the Right PCOS Workup
If you suspect PCOS or have been told you have it but have not had a thorough evaluation, push for these investigations:
- Day 2-3 hormonal panel: FSH, LH, LH:FSH ratio, oestradiol, prolactin, TSH
- Androgens: Total testosterone, free testosterone, DHEAS
- Metabolic panel: Fasting glucose, fasting insulin, HbA1c, lipid profile
- Pelvic ultrasound: To visualise ovarian morphology and endometrial lining
- Mid-luteal progesterone (Day 21 or 7 days post-ovulation): To confirm whether ovulation actually occurred and whether it was adequate
This panel gives a complete hormonal picture and guides whether you need medical ovulation induction or whether lifestyle changes alone are likely to be sufficient. According to guidance from the Indian Council of Medical Research (ICMR) and international reproductive endocrinology bodies like ESHRE, a holistic, stepwise approach – starting with lifestyle, followed by pharmacological ovulation induction when needed – gives the best outcomes for women with PCOS who wish to conceive. You can review ESHRE’s evidence-based PCOS guidelines at eshre.eu for a detailed clinical reference.
The Mental and Emotional Side of PCOS and Fertility in India
This aspect is rarely spoken about openly, yet it profoundly affects outcomes. Indian women with PCOS often face:
- Social pressure to conceive quickly after marriage
- Shame or confusion about irregular cycles
- Anxiety triggered by every missed period
- Misinformation from family, community, or unqualified online sources
Chronic psychological stress, as mentioned earlier, directly worsens PCOS by elevating cortisol and disrupting the HPO axis. This creates a difficult feedback loop: anxiety about fertility worsens PCOS symptoms, which increases anxiety further. Breaking this loop requires:
- Education: Understanding that PCOS usually does not prevent conception entirely, just complicates timing
- Community: Connecting with other Indian women who have PCOS and have conceived
- Professional support: Seeking counselling if fertility anxiety is significantly impacting daily life
- Partnered approach: Involving your partner in cycle tracking and lifestyle changes reduces isolation

Research from the Journal of Human Reproductive Sciences highlights that Indian women with PCOS who received structured psychosocial support alongside medical treatment had significantly better treatment adherence and outcomes than those who received medical treatment alone.
Practical PCOS Cycle Checklist for Indian Women Trying to Conceive
Use this as a monthly reference:
- Record the first day of your period
- Begin BBT tracking from day 1 of your cycle
- Begin checking cervical mucus from day 8 onwards
- Start OPK testing from day 10 (or day 14 if cycles are longer than 35 days)
- Time intercourse every 1-2 days during the fertile window
- After the fertile window, watch for the BBT rise to confirm ovulation
- If BBT does not rise in a given cycle, note it and continue tracking the next cycle
- Keep a record of at least 3-6 cycles to show your doctor if needed
- Follow a low-GI, anti-inflammatory diet throughout the month
- Exercise consistently (minimum 150 minutes of moderate activity per week)
- Prioritise 7-8 hours of sleep
- Take any prescribed or recommended supplements consistently
- Schedule a medical review if you have been trying for 6 months (under 35) or 3 months (over 35) without success
Expert Tips for Managing PCOS Ovulation Naturally
- Track for at least three cycles before drawing conclusions. One cycle with no BBT rise does not mean you never ovulate. Patterns emerge over time.
- Do not rely on the calendar method. Standard apps that predict ovulation based on a 28-day cycle are not reliable for PCOS. Use physiological signs instead.
- Address insulin resistance proactively. Even if you are not diabetic, high fasting insulin suppresses ovulation. A functional medicine or endocrinology review can clarify whether you need medication or dietary changes.
- Eat more protein at breakfast. Research shows that a high-protein morning meal reduces insulin and LH levels throughout the day in women with PCOS.
- Limit late-night eating. Circadian disruption worsens insulin resistance. Keep eating windows aligned with daylight hours where possible.
- Avoid extreme exercise. Overtraining elevates cortisol and can further suppress ovulation. Moderate, enjoyable movement is more effective than punishing workouts.
- Reframe the timeline. Many women with PCOS conceive within one to two years of focused management – which, while longer than average, is still a successful natural conception outcome.
- Involve your gynaecologist early. Do not wait until you are desperate. Early ovulation tracking and monitoring can identify problems sooner and allow timely intervention.
Frequently Asked Questions (FAQ)
Does PCOS prevent ovulation completely in every woman?
No. PCOS does not prevent ovulation completely in most women. The majority of those with PCOS experience oligo-ovulation – infrequent or irregular ovulation – rather than a total absence. A smaller subset may experience anovulation (no ovulation) in most cycles, but this is less common and often improvable with treatment.
Can I get pregnant naturally if I have PCOS and irregular periods?
Yes, many women with PCOS conceive naturally. The key is identifying when ovulation does occur by tracking basal body temperature, cervical mucus, and using ovulation predictor kits. Lifestyle changes that improve insulin sensitivity can also restore more regular ovulation.
How do I know if I am ovulating with PCOS?
The most reliable signs are: a positive OPK (detecting the LH surge), egg-white cervical mucus in the days before ovulation, and a sustained rise in basal body temperature after ovulation. Using all three together gives a more accurate picture than relying on any single method.
Does PCOS prevent ovulation completely even with treatment?
Treatment – particularly Letrozole or Metformin – significantly increases ovulation rates in women with PCOS. Studies show ovulation rates of 70-80% per cycle with appropriate ovulation induction therapy. For women who do not respond to oral agents, injectable gonadotropins or IVF are further options.
What is the best diet for PCOS to improve ovulation?
A low-glycaemic, anti-inflammatory diet is best supported by evidence for PCOS. This means replacing refined carbohydrates with complex carbs like dals, oats, and vegetables; including healthy fats from nuts, seeds, and ghee in moderation; and ensuring adequate protein at each meal. This pattern reduces insulin levels and supports more regular ovulation.
How long does it take to get pregnant with PCOS?
This varies widely. Some women conceive within a few months of focused lifestyle changes. Others take one to two years. Women who require ovulation induction medication may achieve pregnancy within a few treated cycles. The timeline depends on PCOS severity, age, partner fertility, and how well the underlying hormonal drivers are addressed.
Is PCOS more common in Indian women?
Studies suggest that PCOS prevalence in India is among the highest globally, with estimates ranging from 9% to 22% of women of reproductive age. Genetic predisposition combined with dietary patterns, sedentary lifestyles, and high rates of insulin resistance in South Asian populations are thought to contribute to this higher prevalence.
Does stress make PCOS worse and prevent ovulation?
Yes. Chronic psychological stress elevates cortisol, which disrupts the hypothalamic-pituitary-ovarian axis and can worsen anovulation in PCOS. Stress management through yoga, sleep, and counselling is a legitimate and evidence-based part of PCOS management.
Does PCOS Prevent Ovulation Completely? What You Should Take Away

To answer the central question clearly: does PCOS prevent ovulation completely? For most women, the answer is no. PCOS creates irregular, unpredictable ovulation – not a permanent absence of it. Understanding this distinction is crucial, because it changes how you approach conception planning.
You are not working with an impossibility. You are working with a more complex cycle that requires sharper tracking, smarter lifestyle choices, and sometimes medical support. Millions of Indian women with PCOS have conceived, and the tools, research, and clinical pathways to support you are better than ever before.
The key actions are clear:
- Learn your body’s ovulation signals
- Track your cycle with physiological methods (BBT, cervical mucus, OPKs)
- Address insulin resistance through diet, exercise, and targeted supplements
- Seek medical evaluation proactively rather than reactively
- Reduce chronic stress and get adequate sleep
If you are ready to take the next step and want structured, evidence-based support for how to conceive naturally with PCOS, Gntro’s resources are designed specifically for Indian women navigating fertility challenges. You do not have to figure this out alone.