Endometriosis is a chronic condition where tissue similar to the uterine lining grows outside the uterus, most often on the ovaries, fallopian tubes, and pelvic lining. In India, it affects roughly one in ten women of reproductive age, yet the average diagnostic delay stretches to 7-10 years because painful periods are normalised as routine. Understanding what endometriosis is and recognising its symptoms early in India is the first step toward protecting both quality of life and future fertility.
If you have ever been told that “period pain is just something women live with,” you are not alone – and that advice may be doing more harm than good. Millions of Indian women quietly endure symptoms that go far beyond ordinary menstrual discomfort, often for a decade or longer, before anyone puts a name to what they are experiencing. This article breaks down what is endometriosis, symptoms India-specific factors that delay diagnosis, and how the condition intersects with fertility – so you can recognise the signs sooner and make informed decisions about your reproductive health. For couples actively working on how to get pregnant, understanding endometriosis is often a missing piece of the puzzle.
What is Endometriosis? A Quick Definition
Endometriosis is a long-term inflammatory condition in which endometrial-like tissue – the kind that normally lines the inside of the uterus – grows in places it should not, such as the ovaries, fallopian tubes, the outer surface of the uterus, or the pelvic peritoneum. Because this misplaced tissue still responds to the hormonal signals of the menstrual cycle, it thickens, breaks down, and bleeds each month, just like the uterine lining does. Unlike the normal lining, however, this blood has no way to exit the body.
Over time, this trapped blood triggers inflammation, scar tissue, and adhesions – bands of fibrous tissue that can bind organs together. This is what produces the hallmark symptoms of chronic pelvic pain, painful periods, and, in many cases, difficulty conceiving.
Quick Answer: How Common Is Endometriosis in India?
Global health researchers estimate that endometriosis affects approximately 10% of women of reproductive age, translating to tens of millions of women across India alone. Because so many cases go undiagnosed, the true number is likely much higher than official estimates suggest.
Why Endometriosis Symptoms Are Often Missed in India
Recognising what endometriosis is and its symptoms in an Indian context requires understanding the cultural, medical, and structural barriers that delay diagnosis. These factors compound one another, turning what could be a straightforward diagnosis into a years-long ordeal.
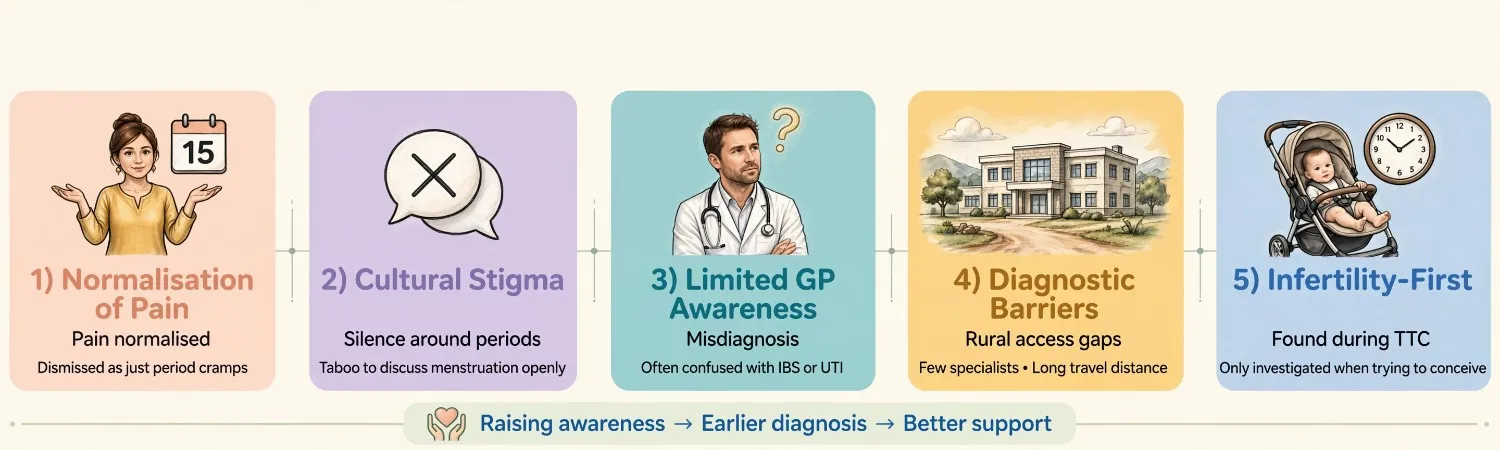
1. Normalisation of Menstrual Pain
From a young age, many Indian women are told that period pain is simply part of being a woman. Phrases like “it happens to everyone” or “it will improve after marriage” discourage women from seeking medical attention for symptoms that are, in fact, abnormal. This normalisation is one of the single biggest reasons diagnostic delay in the region stretches so long.
2. Cultural Stigma Around Menstrual and Reproductive Health
Open conversations about menstrual symptoms, pelvic pain, or painful intercourse remain uncommon in many households. This silence means symptoms are rarely discussed with mothers, sisters, or even friends, let alone flagged to a doctor early.
3. Limited Awareness Among General Practitioners
Endometriosis symptoms – such as heavy bleeding, fatigue, and pelvic pain – overlap with several other gynaecological conditions, including PCOS and adenomyosis. Without specialised training, many general practitioners misattribute these symptoms to “normal” menstrual variation or irritable bowel syndrome, sending women down the wrong treatment path for years.
4. Diagnostic Barriers
A definitive endometriosis diagnosis traditionally requires laparoscopy, a surgical procedure not widely accessible in smaller towns and rural India. With roughly seventy percent of India’s population living outside major cities, many women simply do not have easy access to the gynaecological specialists or imaging equipment needed for early detection.
5. The Infertility-First Presentation
For many Indian women, endometriosis is only discovered when they begin trying to conceive and struggle to do so. Because infertility carries significant social stigma in India, the diagnostic journey often begins under emotional distress rather than routine preventive care – further delaying the connection between symptoms and their underlying cause.
Recognising the Symptoms: What Endometriosis Feels Like
While every woman’s experience differs, there is a consistent cluster of symptoms that should prompt a conversation with a gynaecologist rather than a trip to the pharmacy for painkillers alone.
Core Symptoms Checklist
- Severe dysmenorrhea – period pain intense enough to interfere with work, school, or daily activities
- Chronic pelvic pain – discomfort that persists even outside of menstruation
- Dyspareunia – pain during or after intercourse
- Heavy menstrual bleeding – soaking through pads or tampons faster than expected, or bleeding for longer than seven days
- Premenstrual spotting – light bleeding in the days before a period begins
- Painful bowel movements or urination, particularly during menstruation
- Fatigue, bloating, and digestive discomfort, sometimes mistaken for IBS
- Difficulty conceiving after several months of regular, unprotected intercourse
A Simple Way to Tell the Difference
A helpful rule of thumb: ordinary period cramps typically respond to over-the-counter pain relief and do not stop you from going about your day. Endometriosis-related pain frequently does not respond well to standard painkillers and can be severe enough to cause missed work or school days, month after month.
| Feature | Typical Period Pain | Possible Endometriosis Pain |
|---|---|---|
| Onset | Starts with bleeding, eases in a day or two | Can begin days before bleeding starts |
| Intensity | Manageable with rest or mild medication | Often severe, disrupts daily activities |
| Response to painkillers | Usually improves | Frequently persists despite medication |
| Timing | Limited to menstruation | Can occur throughout the cycle |
| Associated symptoms | Mild bloating, fatigue | Pain during sex, bowel or urinary symptoms, heavy bleeding |
| Trend over time | Stable or improves with age | Often worsens progressively without treatment |
If several of these patterns sound familiar, it is worth raising them directly and specifically with a gynaecologist, rather than describing them simply as “bad periods.”
World Health Organization – Endometriosis fact sheet
What Causes Endometriosis?
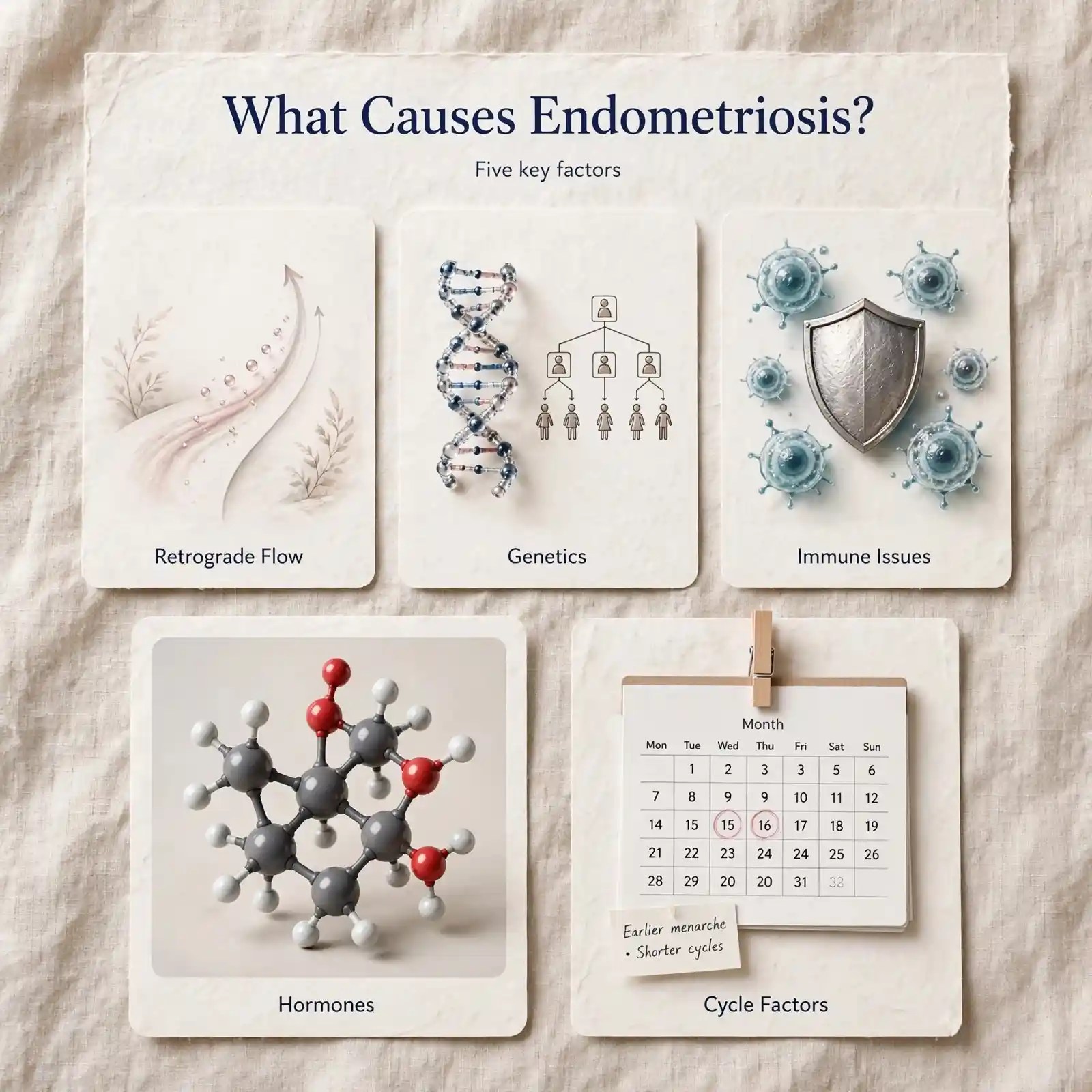
The exact cause of endometriosis is not fully understood, but researchers point to several contributing theories:
- Retrograde menstruation – menstrual blood flowing backward through the fallopian tubes into the pelvic cavity instead of leaving the body
- Genetic predisposition – a family history of endometriosis raises individual risk
- Immune system dysfunction – an impaired ability to recognise and clear misplaced endometrial tissue
- Hormonal factors – oestrogen appears to fuel the growth of endometrial-like tissue
- Early menarche or shorter menstrual cycles – some studies link earlier onset of periods and shorter cycle length with higher endometriosis risk
None of these factors alone fully explains why endometriosis develops, and ongoing research continues to investigate genetic and environmental contributors.
How Endometriosis Affects Fertility
One of the most pressing concerns for Indian women is the relationship between endometriosis and the ability to conceive. Not every woman with endometriosis experiences fertility challenges, but the condition is a recognised contributor to difficulty conceiving.
The Mechanisms Behind Reduced Fertility
- Distorted pelvic anatomy – scar tissue and adhesions can physically block or distort the fallopian tubes, interfering with the egg’s path to the uterus
- Inflammatory environment – chronic inflammation in the pelvic cavity can affect egg quality, sperm function, and embryo implantation
- Ovarian reserve impact – endometriomas (cysts formed by endometrial tissue on the ovaries) can reduce the number and quality of available eggs
- Altered hormonal signalling – inflammation may interfere with the coordinated hormonal changes required for ovulation and implantation
Staging and What It Means for Conception
Doctors typically classify endometriosis into four stages, from minimal to severe, based on the extent and location of tissue growth:
| Stage | Description | General Fertility Impact |
|---|---|---|
| Stage I (Minimal) | Small, superficial lesions | Often limited impact on natural conception |
| Stage II (Mild) | More lesions, still superficial | Mild reduction in fertility likelihood |
| Stage III (Moderate) | Deeper lesions, small endometriomas, some adhesions | Noticeable reduction; may need medical support |
| Stage IV (Severe) | Deep lesions, large endometriomas, dense adhesions | Significant impact; often requires specialised fertility treatment |
Importantly, the stage of endometriosis does not always match the severity of pain a woman experiences – some women with minimal disease have debilitating pain, while others with more extensive disease report milder symptoms. This is one more reason self-diagnosis based on pain level alone is unreliable, and professional evaluation matters.
If you are trying to conceive and suspect endometriosis may be a factor, timing intercourse correctly around ovulation becomes even more important. Our guide on the best time to have intercourse to conceive walks through how to identify your fertile window with greater precision.
Getting an Accurate Diagnosis
Because symptoms overlap with other conditions, an accurate diagnosis typically involves a combination of approaches:
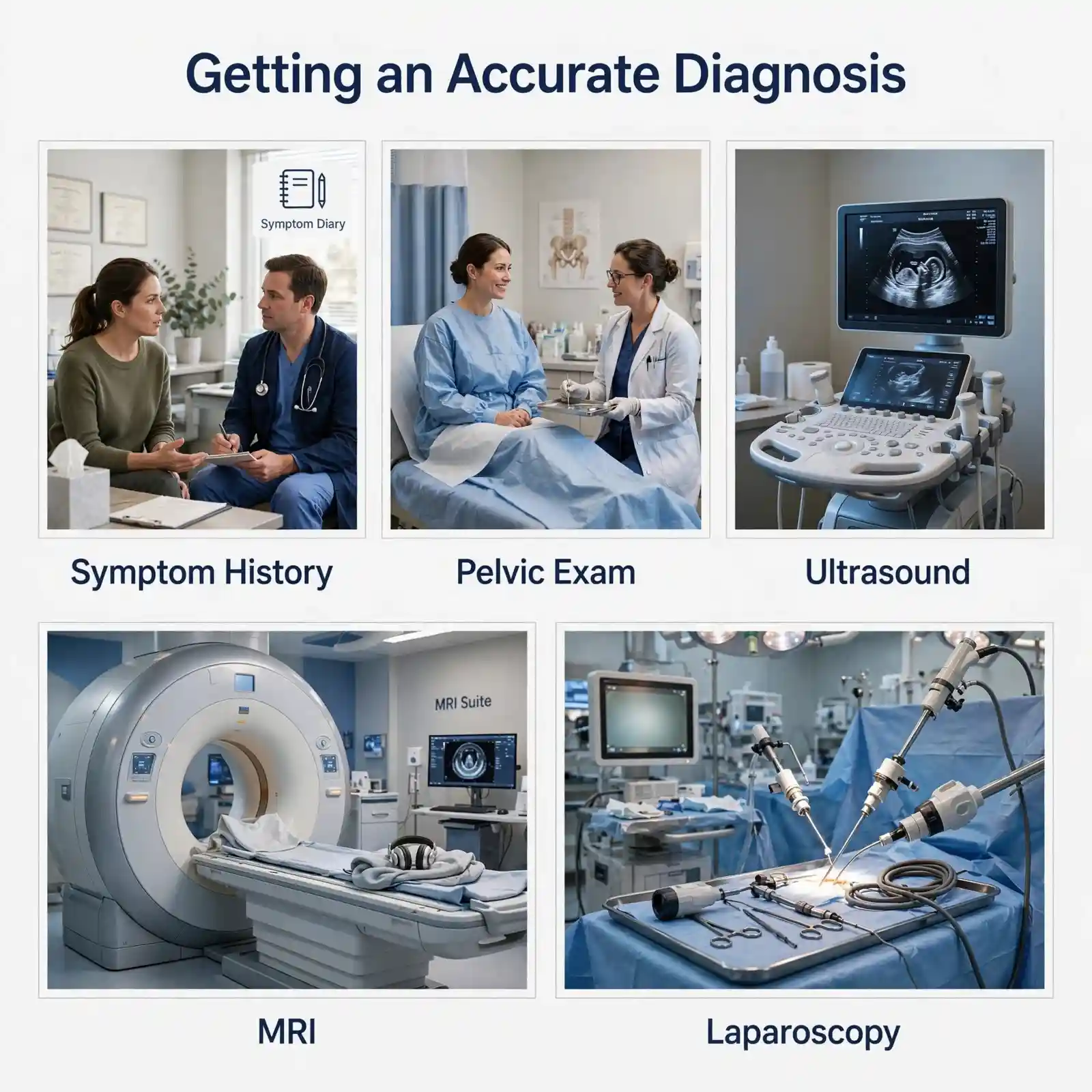
- Detailed symptom history – a thorough discussion of pain patterns, cycle characteristics, and family history
- Pelvic examination – to check for tenderness, cysts, or nodules
- Transvaginal ultrasound – useful for identifying ovarian endometriomas, though it cannot detect all forms of the disease
- MRI – can help map deeper infiltrating lesions in complex cases
- Laparoscopy – still considered the definitive diagnostic method, allowing direct visualisation and, often, simultaneous treatment of lesions
Many women benefit from starting with a detailed symptom diary before their appointment, tracking pain intensity, cycle length, bleeding patterns, and any digestive or urinary symptoms across two to three cycles.
This concrete record helps a gynaecologist distinguish endometriosis from conditions like PCOS more efficiently. If PCOS is also a concern, our article on whether PCOS always stops ovulation in the Indian woman’s cycle explains how the two conditions can sometimes be confused – or coexist.
Common Mistakes Women Make When Dealing With Endometriosis Symptoms
- Waiting too long to seek help – assuming pain will simply resolve on its own or after marriage or childbirth
- Relying solely on painkillers – masking symptoms without addressing the underlying cause delays proper treatment
- Not tracking cycle patterns – without a record, it becomes harder to communicate symptom severity accurately to a doctor
- Assuming a normal ultrasound rules out endometriosis – many forms of the disease do not show up clearly on standard ultrasound
- Ignoring the fertility connection – not raising conception concerns proactively with a gynaecologist, even when trying to conceive for over six months
- Skipping nutritional support – overlooking the role of an anti-inflammatory, nutrient-dense diet in managing symptoms and supporting fertility
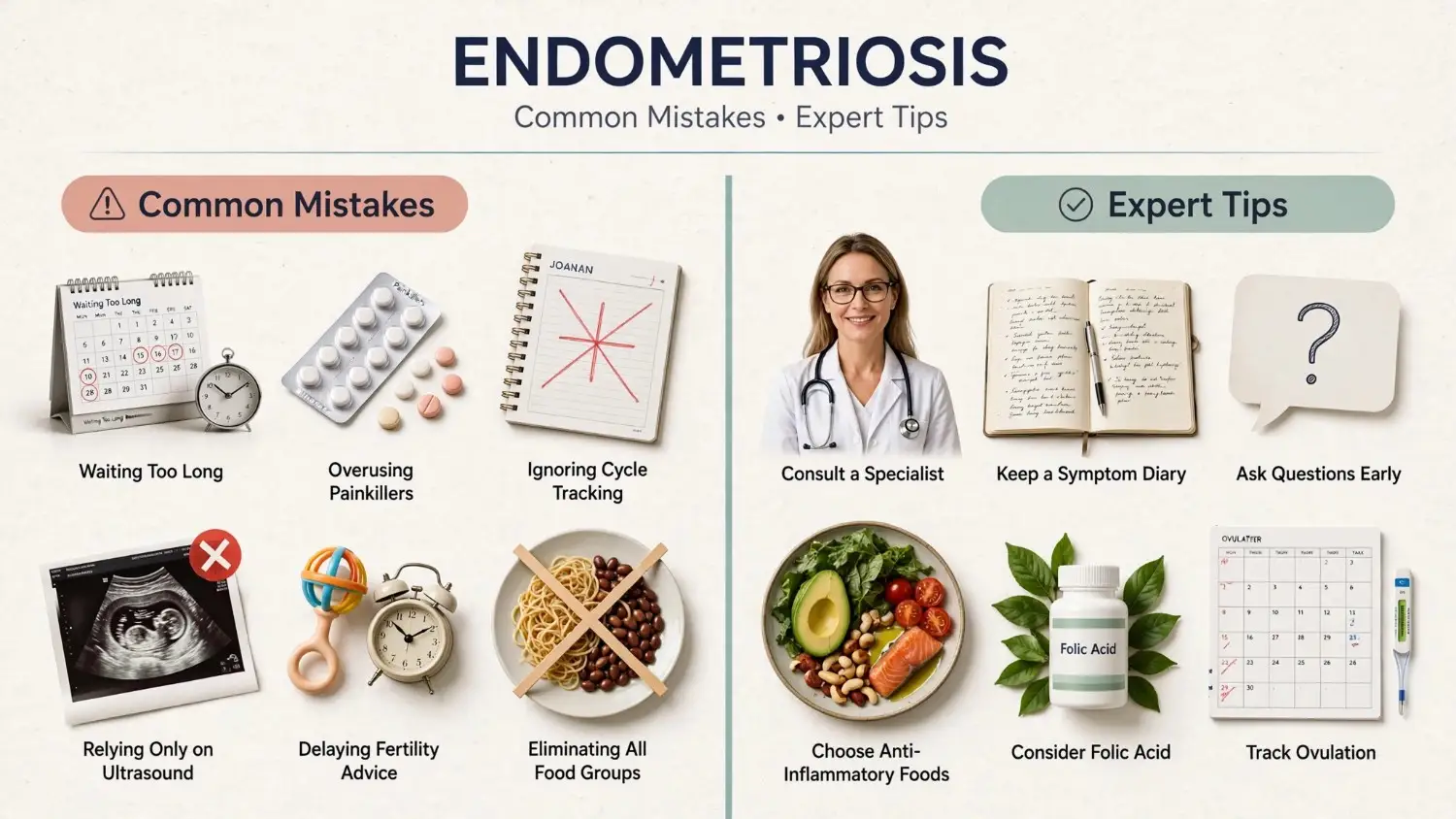
Expert Tips for Managing Symptoms and Supporting Fertility
- Seek a gynaecologist familiar with endometriosis specifically, rather than a general practitioner alone, if symptoms persist beyond two or three cycles
- Keep a symptom and cycle diary for at least two to three months before your appointment
- Ask directly about endometriosis during consultations, rather than only describing pain in general terms
- Prioritise an anti-inflammatory diet rich in folate, omega-3 fatty acids, and antioxidants, which may help manage inflammation. Our detailed fertility diet meal plan guide offers a structured approach
- Don’t overlook micronutrients like folic acid, which play a role in reproductive health regardless of an endometriosis diagnosis; see our list of Indian food sources of folic acid for women trying to conceive
- Discuss fertility preservation early if you are diagnosed with moderate to severe endometriosis and are not yet ready to conceive
- Understand your ovulation window precisely, since timing becomes more critical when any fertility-limiting factor is present. Our guide on ovulation and conception – what exactly happens, step by step breaks the process down clearly
Treatment Options at a Glance
| Approach | What It Involves | Best Suited For |
|---|---|---|
| Pain management | NSAIDs, hormonal therapy to suppress lesion activity | Symptom control, not actively trying to conceive |
| Hormonal therapy | Birth control pills, progestins, GnRH agonists | Reducing lesion growth and pain, non-conception phase |
| Laparoscopic surgery | Removal or ablation of endometrial lesions and adhesions | Moderate to severe disease, fertility-focused cases |
| Assisted reproduction | IUI or IVF depending on severity and other factors | Cases where natural conception is significantly affected |
| Lifestyle and diet support | Anti-inflammatory nutrition, stress management, regular movement | Complementary support alongside medical treatment |
Treatment decisions depend heavily on the stage of the condition, symptom severity, age, and whether conception is an immediate goal – which is why a personalised consultation with a specialist remains essential rather than relying on general information alone.
Endometriosis Myths vs Facts in India
Misinformation around endometriosis spreads quickly in a culture where menstrual health is rarely discussed openly. Separating myth from fact is a crucial part of understanding what endometriosis is and why its symptoms deserve serious attention.
| Myth | Fact |
|---|---|
| “Severe period pain is normal for every woman” | Debilitating pain that disrupts daily life is not typical and should be evaluated by a doctor. |
| “Endometriosis only affects older women” | It commonly begins in the teenage years, often shortly after the first period. |
| “Getting pregnant cures endometriosis” | Pregnancy may temporarily ease symptoms, but the underlying condition can return afterward. |
| “A normal ultrasound means there is no endometriosis” | Many lesions, especially superficial ones, do not appear clearly on standard ultrasound. |
| “Endometriosis always means infertility” | Many women with mild to moderate disease conceive naturally, sometimes with minor support. |
| “Painkillers are enough to manage it” | Painkillers mask symptoms but do not slow disease progression or address the underlying inflammation. |
| “Only women with a family history get it” | While genetics play a role, endometriosis can occur without any known family history. |
Step-by-Step: What to Do If You Suspect Endometriosis
If several of the symptoms described above sound familiar, here is a practical sequence to follow rather than waiting for the pain to resolve on its own:
Step 1: Start a symptom diary today.
Note pain intensity (on a scale of one to ten), bleeding volume, cycle length, and any digestive, urinary, or intercourse-related discomfort for at least two full cycles.
Step 2: Book a consultation with a gynaecologist.
Ideally one with experience managing endometriosis or chronic pelvic pain specifically, rather than a general physician alone.
Step 3: Bring your diary and be specific.
Rather than saying “my periods are painful,” describe how the pain compares to before, how it affects your daily routine, and whether painkillers help.
Step 4: Ask directly whether endometriosis should be ruled out
Request a transvaginal ultrasound as a starting diagnostic step.
Step 5: Discuss your fertility goals openly
Even if pregnancy is not an immediate plan, so any treatment chosen also considers your long-term reproductive intentions.
Step 6: Follow up on next steps
Whether that means hormonal management, further imaging like an MRI, or a referral for laparoscopic evaluation.
Step 7: Revisit your nutrition and lifestyle habits
Alongside medical treatment, since anti-inflammatory support can complement – though never replace – a proper clinical management plan.
Taking these steps early, rather than after years of unexplained pain, is one of the most effective ways to protect both quality of life and future fertility potential.

Living With Endometriosis: Beyond the Physical Symptoms
Endometriosis is not only a physical condition – it carries emotional weight too. Chronic pain and fertility uncertainty are linked with higher rates of anxiety and stress among affected women. Building a support system, whether through a partner, family, or a patient community, can make a meaningful difference in coping with the day-to-day and long-term aspects of the condition. Speaking openly with a trusted gynaecologist about both the physical and emotional dimensions of the diagnosis is an important part of comprehensive care.
Frequently Asked Questions
What is endometriosis, and what are its main symptoms in India?
Endometriosis is a condition where uterine-like tissue grows outside the uterus, causing inflammation and pain. Common symptoms in Indian women include severe period pain, heavy bleeding, pelvic pain outside menstruation, pain during intercourse, and difficulty conceiving.
At what age does endometriosis usually appear?
Endometriosis most often appears between the teenage years and menopause, with many women first noticing symptoms in their late teens to early thirties, though diagnosis is frequently delayed well beyond symptom onset.
Can endometriosis be cured completely?
There is currently no permanent cure for endometriosis, but a combination of hormonal therapy, surgery, and lifestyle adjustments can manage symptoms effectively and, for many women, support successful conception.
Does every woman with endometriosis struggle to conceive?
No. Fertility impact varies significantly by stage and individual factors. Many women with mild endometriosis conceive naturally, while those with moderate to severe disease may need additional medical support.
How is endometriosis different from PCOS?
Endometriosis involves tissue growth outside the uterus and is linked to inflammation and pelvic pain, while PCOS is a hormonal condition affecting ovulation. The two can share some symptoms, such as irregular cycles, but require different diagnostic approaches and treatments.
What tests confirm an endometriosis diagnosis?
While ultrasound and MRI can suggest endometriosis, laparoscopy remains the most definitive diagnostic method, allowing doctors to directly view and, in many cases, treat lesions during the same procedure.
Can diet help manage endometriosis symptoms?
An anti-inflammatory diet rich in vegetables, omega-3 fatty acids, and key micronutrients like folate may help reduce inflammation and support overall reproductive health, though it is not a replacement for medical treatment.
Why does endometriosis take so long to diagnose in India?
Diagnostic delay in India stems from a combination of normalised period pain, cultural stigma around discussing reproductive symptoms, limited awareness among general practitioners, and restricted access to specialists and laparoscopic facilities outside major cities.
Does having endometriosis mean I will need IVF to conceive?
Not necessarily. Many women with mild to moderate endometriosis conceive through natural or minimally assisted methods, particularly with precise ovulation timing. IVF or other assisted reproductive technologies typically become more relevant for moderate to severe stages or when other fertility factors are also present.
Taking the Next Step
Understanding what endometriosis is and recognising its symptoms early can meaningfully change the course of both symptom management and fertility outcomes for Indian women. Rather than normalising severe period pain or delaying a conversation about fertility concerns, timely awareness and specialist consultation remain the most powerful tools available. If you are navigating a diagnosis or simply trying to understand your body better while planning a pregnancy, tailored to your unique fertility journey.